
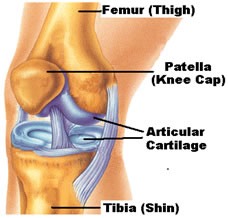
The knee joint is lined with articular cartilage. This is a very smooth surface that is more slippery than ice. The back of the knee cap is also lined with articular cartilage.
Damage to the articular cartilage can lead to pain, catching, locking and a feeling of instability of the knee joint. Damage can be partial or full thickness and can be isolated to one area or generalized .
Osteoarthritis (wear and tear arthritis) is an example of generalized cartilage damage that can result from trauma or can occur without obvious cause. Isolated articular cartilage defects often arise from trauma or sometimes an underlying bone disorder. When the articular cartilage is damaged pieces can flake off and form loose bodies floating in the joint. These can grow larger with time and can be responsible for the joint jamming.

At the time of arthroscopy (keyhole surgery) the following procedures can be performed.
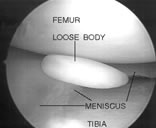
1. Removal of Loose Bodies
If a loose body is identified it can be removed. Occasionally this requires an extra small incision (depending on the size of the loose body). Loose bodies in the back of the knee can require extra portals. Sometimes even though loose bodies are seen on x-rays and scans before surgery they can be impossible to locate at arthroscopy.
2. Joint Debridement (Chondroplasty)
Trimming and smoothing loose flaps of articular cartilage (chondroplasty) can be useful in partial thickness damage or generalized damage. In appropriately selected patients a joint debridement can improve arthritic symptoms for 2 years in up to 70 out of every 100 patients. Chondroplasty does not fix the underlying damage but attempts to minimise the symptoms it causes.
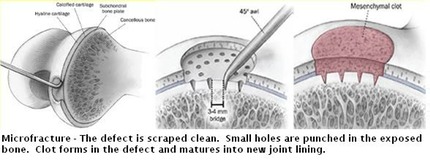
3. Microfracture
This technique encourages cartilage regeneration. It is useful in isolated defects that are full thickness. It involves punching small holes in the bone exposed by the missing cartilage. These holes allow marrow and stem cells to leak from the bone into the defect. A clot forms which converts to a healing cartilage.
While not as resilient as normal articular cartilage this repair type cartilage enables the joint to function more closely to normal.
Microfracture is heavily dependent on rehabilitation for success. It usually involves being non weight bearing (on crutches) for 6 weeks. Kneecap lesions can weight bear but are in a limited range of motion knee brace for 6 weeks. Rehabilitation takes 6 months.
4. Do Nothing
Minor partial thickness articular cartilage damage is quite a common finding at arthroscopy. If the location of the damage does not match the patient’s symptoms or if there are no loose fragments then often the best treatment is to leave well alone
Damaged articular cartilage is not a life threatening condition and surgery is always optional, never essential. Some damage may be noticed at the time of arthroscopy but may not be causing any symptoms. Damage in some patients will become progressively worse while in others will stay the same for years. Some damage is too severe to treat arthroscopically and requires other strategies such as joint replacement. Remember the decision to proceed to surgery is the patients.